Content by: Mrunmayee Nerlikar, Saachi Kurudi
Design by: Manan Chawda
As our lifestyles become more modern and life expectancies skyrocket, we are bearing witness to increasing rates of “Western” diseases among our population. Quite prominent among these diseases is cholelithiaisis, or gallstones. Classically described to occur in the fat, fertile female of forty, research now shows that gallstones can be found in up to 3-5% of adults in India, and children are being increasingly affected. As the rates of this relatively simple disease rise, it might be prudent to expect an increase in some of its rarer complications, and this discussion is about the rarest of them all- Bouveret Syndrome.
With non-specific symptoms and laboratory findings,high mortality rates and only 315 reported cases between 1967 and 2016, Bouveret Syndrome is a rare complication of gallstone disease, in which a bilioenteric fistula causes a gallstone, typically 2-8 cm in size, to pass from the gallbladder into the stomach or duodenum, leading to a gastric outlet obstruction.
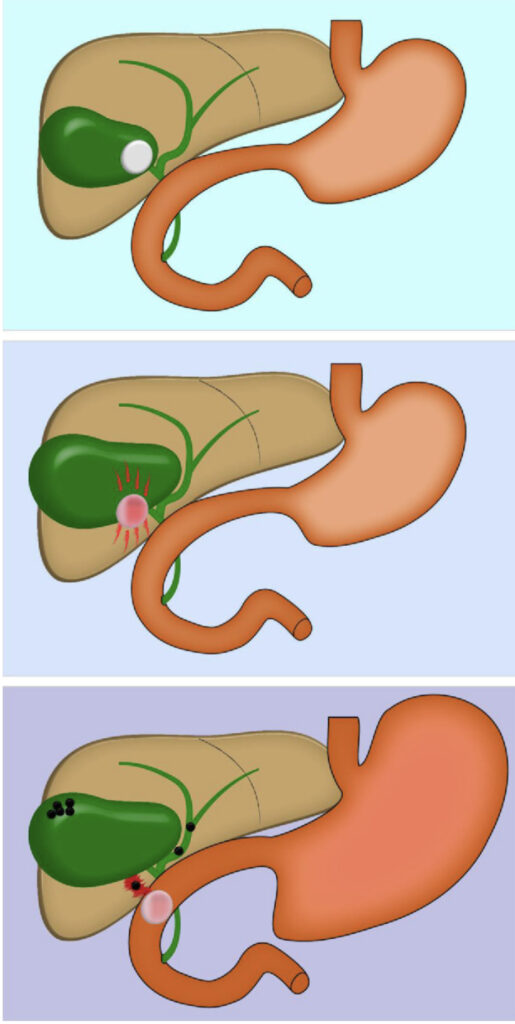
With such a thick walled gallbladder, how does such a connection even form, you may wonder?
The inflammation of gallbladder along with the mechanical pressure of gallstones on the bowel wall, following an attack of acute cholecystitis, may cause an ischemic tear of the gallbladder and intestinal wall. This facilitates the formation of a fistula between the two organs where the gallstone could easily pass.
The presentation of such patients is highly variable, and clinical findings non-specific. Most commonly described is a triad of epigastric pain, nausea and vomiting. Other common non-specific signs are abdominal tenderness, dehydration, abdominal distention, upper gastrointestinal hemorrhage with hematemesis, and pyrexia. One third of patients present with jaundice and hepatic enzyme alteration. Depending on the intensity of inflammatory response, there may be leukocytosis, electrolyte abnormalities, acid-base alterations, and renal failure.
With such a non-specific presentation and the rather elderly and co-morbid group of patients that this complication presents in, time is of the essence and an early diagnosis is crucial. In such a situation, imaging modalities seem to be a logical first step.
Maybe an abdominal radiograph?
Findings may include pneumobilia, intestinal obstruction, aberrantly located gallstone, air-fluid levels in the right upper quadrant due to air in the gallbladder, gastric distention, and a change in the location of a previously observed stone.
Mention needs to be made of course, of the Rigler’s triad described by Leo Geore Rigler in 1940, which talks about the three findings of pneumobilia (air in the biliary tree), bowel obstruction and an aberrant gallstone, which although is highly specific is present in only 40-50% of cases. In such a scenario, CT scan becomes the imaging modality of choice, with close to 100% accuracy. It also provides information regarding presence of fistula, inflammation of the surrounding lumen and tissue , size of gallstone and number of gallstones.

Alright, so we have diagnosed Bouveret syndrome, a rare complication of a fairly common disease. But the story hardly ends there, does it? In fact, it has only just begun. A rare complication, while interesting to diagnose, is also much less studied, and guidelines for management are hard to come by. Management therefore, falls at the surgeon’s discretion.
Initial decompression of the stomach by insertion of a nasogastric tube is often carried out to relieve symptoms. Endoscopic or percutaneous management may be tried initially, but it has been found that over 90% of patients end up requiring surgery.
Surgical options include the following-
Enterolithotomy, where in the aberrant stone is removed through an enterotomy (an opening in the intestine) without touching the enterobiliary fistula.
Cholecystectomy (removal of gallbladder) with fistula repair.
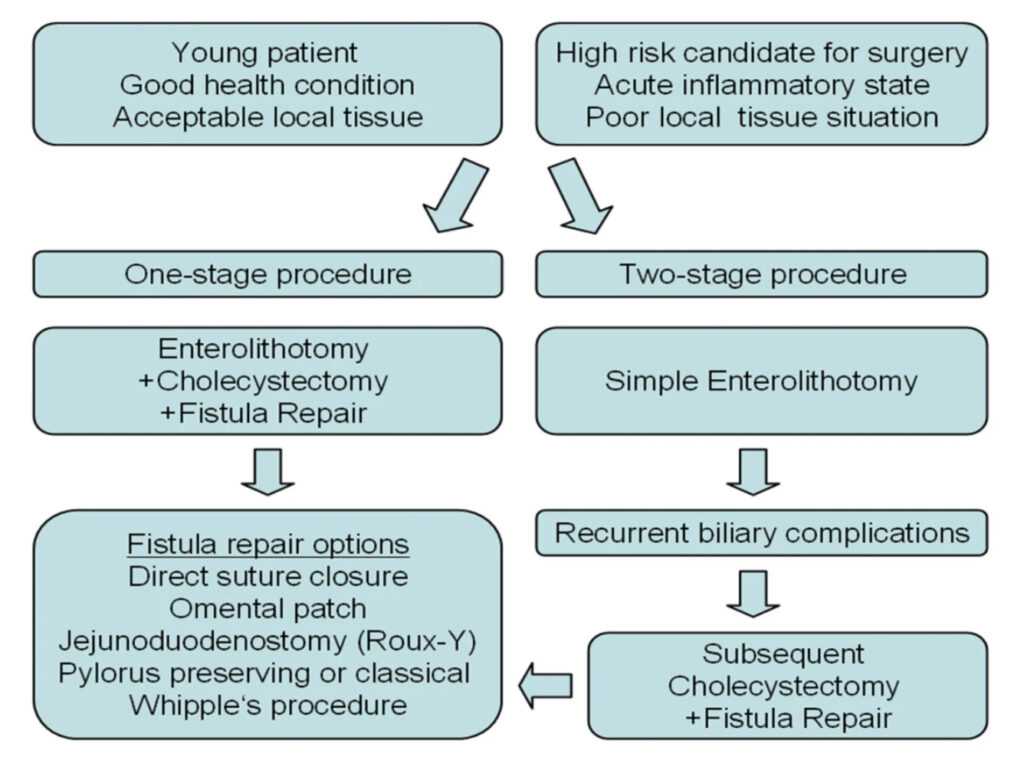
These procedures can be done individually, or combined into a single long procedure- which depends largely on the patient’s status.
So while an elderly patient with multiple comorbidities might benefit from only an enterolithotomy, in a younger fitter patient, a combined procedure may be more fruitful to prevent future recurrence. This is just one example of the nuances that go into the management decisions a surgeon must make on a day to day basis.
Some common complications include ongoing gastric outlet obstruction, which further results in anorexia, nutritional deficiencies, dehydration and electrolyte abnormalities. One of the fatal complications is intestinal perforations.
Sources: Turner AR, Kundaravalli P, Al-Musawi JH, et al. Bouveret Syndrome (Bilioduodenal Fistula) [Updated 2023 Mar 13]. In: StatPearls [Internet]. Treasure Island (FL) : StatPearls Publishing; 2023 Jan-.