Content by: Elvin Joshua Pinto, Keertana
Design by: Chandini K M
Webpost by: Saachi Kurudi

Fetus in fetu (FIF) is an exceptionally rare congenital anomaly where a malformed, parasitic twin is found within the body of its host twin. The anomaly is thought to result from aberrant embryogenesis, where one twin becomes enveloped by the other during early development.
Pathogenesis and Embryological Origin
FIF arises due to an aberration during early embryonic development. During the ventral folding of the trilaminar embryonic disc in the second to third weeks of development, a diamniotic monochorionic twin becomes included within its sibling’s body. This results from unequal division of the totipotent inner cell mass, where one twin’s growth dominates, effectively enveloping the other.
Unlike teratomas, which arise from pluripotent germ cells and lack systemic organization, FIF displays an organized structure, often with a vertebral axis and rudimentary organogenesis. These characteristics underscore its origin from a monozygotic diamniotic twin that failed to fully develop.
Clinical Presentation
FIF commonly presents in infancy as an abdominal mass. Key symptoms include:
- Abdominal distension
- Failure to thrive
- Palpable mass
- Feeding difficulties
Rarely, FIF is discovered later in life, with cases reported in adults as old as 36 years. Associated findings may include cryptorchidism, developmental delay, or urinary obstruction due to mass effects.
Case Study
An 18-month-old male presented with a distended abdomen and failure to thrive. Imaging revealed a retroperitoneal mass containing calcifications, a vertebral column, and budding limbs—hallmark features of FIF. Surgical resection confirmed the diagnosis, and histopathologic examination identified benign tissue consistent with an anencephalic parasitic twin. Postoperative recovery was uneventful, underscoring the curative potential of complete excision.
Differentiating FIF from Teratoma
While FIF and mature teratomas may appear similar, key distinctions exist:
1. Vertebral Axis: FIF typically contains a vertebral column, indicating advanced embryonic development, while teratomas lack this structure.
2. Tissue Differentiation: FIF displays organized, highly differentiated tissues. Teratomas, by contrast, show haphazard collections of tissues from all three germ layers.
3. Growth Potential: Teratomas exhibit independent growth and a risk of malignancy (up to 10% for retroperitoneal teratomas), whereas FIF is benign and non-autonomous.
Diagnostic Approaches
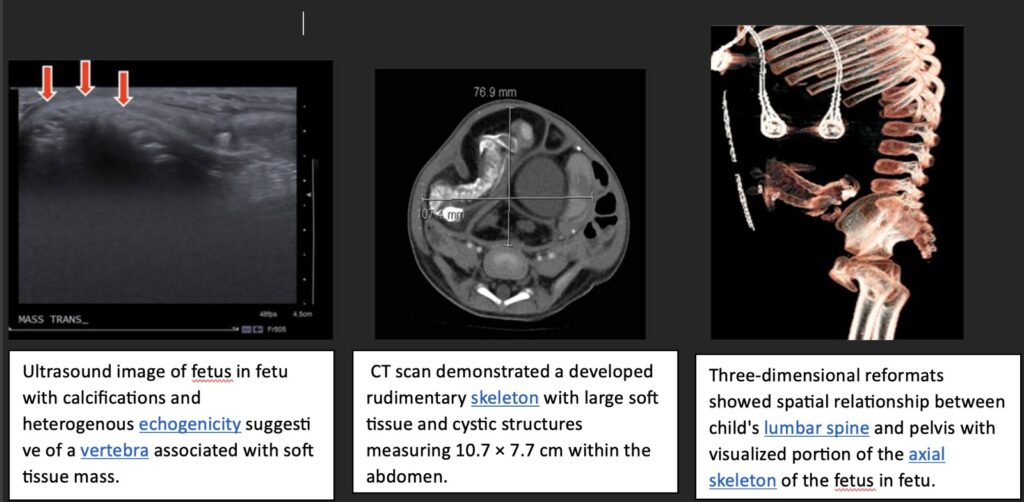
Modern imaging modalities have revolutionized the diagnosis of FIF. Prenatal ultrasonography can identify masses suggestive of FIF, with advancements in computed tomography (CT) and magnetic resonance imaging (MRI) providing detailed insights into the anatomy and spatial relationships of the mass. Three-dimensional reconstructions further aid surgical planning.
Histopathologic examination remains the gold standard for definitive diagnosis, confirming the presence of organized tissues and ruling out malignancy.
Management and Prognosis
Surgical excision is the definitive treatment for FIF. Key surgical considerations include:
- Identification and preservation of vital structures displaced by the mass.
- Complete resection to prevent recurrence and alleviate symptoms.
Postoperative outcomes are typically excellent, with most patients experiencing resolution of symptoms and normal development. However, isolated reports of malignancy associated with FIF or concurrent teratomas emphasize the importance of long-term follow-up. Monitoring tumor markers, such as alpha-fetoprotein (AFP) and human chorionic gonadotropin (HCG), for at least two years postoperatively is recommended.
Pathological and Genetic Insights
Genetic studies of FIF have revealed that its karyotype is identical to that of the host, confirming its monozygotic origin. Advances in molecular analysis have further elucidated the embryological mechanisms underlying this condition, providing insights into its differentiation from teratomas.
Conclusion
Fetus in fetu is a captivating anomaly that offers invaluable lessons in embryology, pathology, and clinical care. While rare, its diagnosis and management underscore the importance of multidisciplinary collaboration and the role of advanced imaging and surgical expertise. For medical students, FIF serves as a testament to the complexities of human development and the marvels of modern medicine.
Reference
https://www.sciencedirect.com/science/article/pii/S2213576615300208