Article by : Vartika, Pradnayan and Vaishnavi
Design by : Utkarsh Agrawal
A 73 year old woman walks in with the complaint of pain for 2 years, worsening over the past 2 weeks.
It was found out that she has had multiple sclerosis for 6 years. Initially she responded to oxcarbamazone but when the pain recurred, pregabalin was added. However, this gave her side effects of somnolence(excessive sleepiness) and dizziness.
At the time of presentation, her pain was sharp, shooting and severe in intensity and lasting for approximately 20 to 30 seconds. It was triggered by trivial daily activities like touching, brushing, chewing and washing the face. She was completely pain free in between the attacks of pain, which had the frequency of about 40 to 50 per day.
A contrast-enhanced magnetic imaging resonance (MRI) scan confirmed the diagnosis of Multiple Sclerosis with plaques involving root entry zones of both the trigeminal nerves.
As the pain couldn’t be resolved through medical treatment, the patient was offered Radio Frequency Ablation (RFA).
What does Radio frequency Ablation really do? Here’s the procedure!
(Patients are fasted for at least 6 h before the procedure. Prophylactic antibiotic is administered 1 h before the procedure. Intravenous access is obtained, and standard monitors including electrocardiogram, blood pressure monitoring, and pulse oximetry are applied. Sedation is usually necessary to increase patient comfort and reduce anxiety.)
- 1. The procedure is performed under fluoroscopic guidance with the patient in the supine position and head extended. The C-arm is rotated to obtain an oblique submental view to visualize the foramen ovale. The skin entry point is ~2–3 cm lateral to the commissura labialis (angle of the mouth) on the affected side. The needle trajectory follows a straight line directed toward the pupil when seen from the front and passes 3 cm anterior to the external auditory meatus when seen from the side.
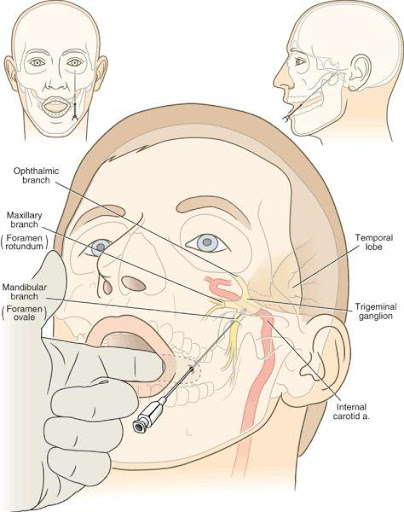
- 2. A 22-gauge, 10-cm RF cannula with a 5-mm active tip is used. After administration of local anesthesia, the cannula is advanced in a coaxial manner (tunnel view) to the X-ray beam toward the foramen ovale. A finger can be placed in the oral cavity to make sure that the buccal mucosa has not been perforated.
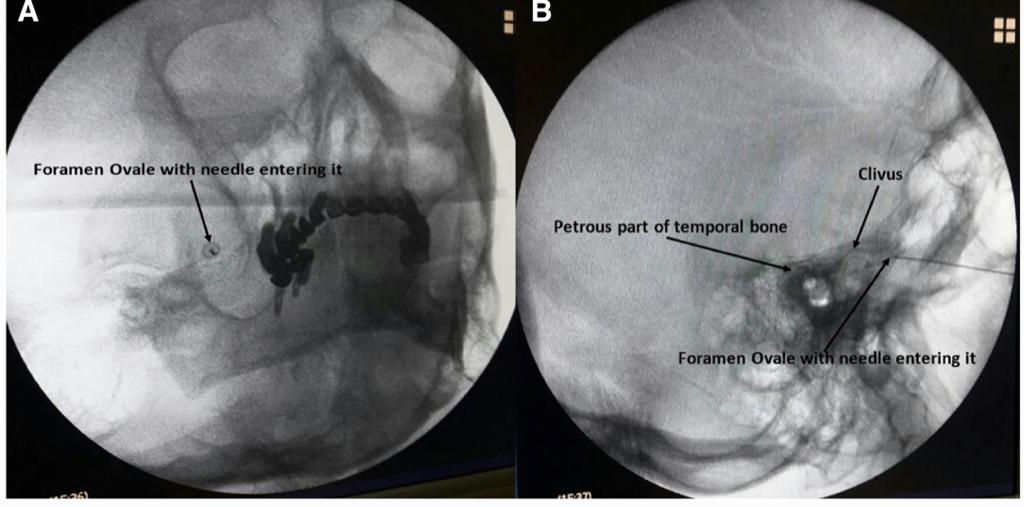
- 3. When the cannula enters the foramen ovale, the depth of the cannula inside the Meckel’s cavity is ascertained on the lateral fluoroscopic view. The electrode is advanced ~2–4 mm further through the canal of the foramen ovale such that the tip of the electrode reaches the junction of the petrous ridge of the temporal bone and the clivus. The stylet is then removed from the cannula, and aspiration is performed to ensure that there is no CSF or blood. Injecting 0.5 mL contrast dye helps to confirm that the needle has not penetrated the dura.
- 4. Test stimulation is mandatory before RF lesioning. The mandibular nerve lies in the lateral portion of the foramen ovale. If the nerve is stimulated at 2 Hz between 0.1 and 1.5 Hz, muscle contraction of the lower jaw may be seen. This confirms that the needle has passed through the foramen ovale and the tip is lying on the trigeminal roots.
- 5. Next, paresthesia in the concordant trigeminal distribution of the patient’s usual symptoms (V1, V2, or V3 divisions) at 50 Hz, 1 msec pulse duration should be reproducible at 0.1–0.5 V.28,29 If paresthesia is only obtained above 0.5 V stimulation, the needle should be redirected to get the same response at a lower voltage.
- 6. After appropriate stimulation parameters have been achieved, 0.5 mL of 0.25% bupivacaine with 40 mg of triamcinolone should be injected. After waiting for at least 30 sec, RF lesioning at 60°C is carried out for 60 sec. The needle can be repositioned to repeat RF lesioning if more than one branch of the trigeminal nerve is involved