Article by: Utkarsh Agrawal and Alisha Lobo
Design by: Alisha Lobo
A seemingly healthy 31 year old woman G3P3 was complaining of lower abdominal pain lasting more than 2 weeks.
The pain was describe to be mild to moderate pain. She had a Cu IUD and reported regular periods. The IUD was found within the uterine cavity, but the strings were not visible for removal
Vaginal discharge without bleeding was discovered upon physical examination, along with a tender Uterus and adnexa upon bimanual palpation.
Other findings include:
Endometrial lining of 5mm
Bilaterally normal ovaries with some fluid in the right fallopian tube
No fluid in pouch of Douglas.
Biochemical Findings:
Temperature: 36.7
Serum CRP 100g/L
Beta-hCG was 412mIU/ml
Initial diagnosis of pelvic infection and prescription of doxycycline and metronidazole was given.
Two days later, patient discovered blood on toilet paper. She also reported an increase in pain. A gynaecological examination revealed a retro-uterine fixed tender mass, which was confirmed using a transvaginal ultrasound. The scan revealed a 6x5cm mass with hypoechoic and anechoic areas.
Fresh blood was found after performing a rectal examination. As a result, a rectoscopy was performed, which revealed a 1.5 cm perforation in the anterior rectal wall, surrounded by actively bleeding tumour-like tissue located 145 cm from anal verge.
Lab examinations revealed increased serum CRP to 179 g/L while beta-hCG decreased 366 mIU/mL. Hemoglobin was 11.5g/100 mL.
A laparoscopy performed after the rectoscopy showed pelvic adhesions, which were removed to reveal the right uterine tube in the pouch of Douglas, with an ampullary dilation of 5 cm. A salpingo-oophorectomy of the right uterine tube and ovary was performed and the rectal perforation was sutured.
Serum beta-hCG levels dropped to undectable levels 5 days post-op.
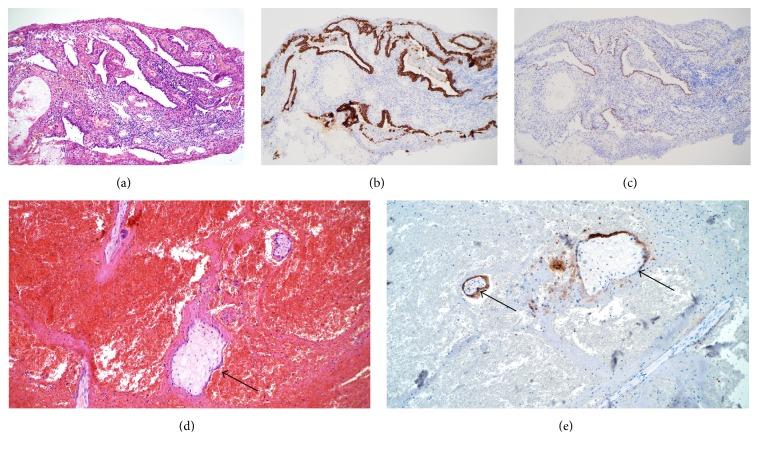
Biopsies of the sample of the mass and the uterine tube confirmed a chronic ectopic pregnancy with no signs of malignancies.
Case Discussion:
Rectal bleeding is a extremely rare complication of rectal ectopic pregnancy. Other parts of the GI tract that are commonly associated with bleeding in cases of ectopic pregnancies include the terminal ileum, sigmoid colon and caecum.
The patient had a chronic ectopic pregnancy that was confirmed by histopathological examination. These cases are known to present with lower abdominal pain and vaginal bleeding.
The dissolution of the tubal wall due to growth of the trophoblastic tissue and the subsequent destruction that ensues has been the popular hypothesis behind a chronic ectopic pregnancy. As a result, slow leakage of blood into the peritoneal cavity, along with trophoblastic tissue and the damaged tubal tissue triggers an inflammatory reaction leading to formation of adhesions.
The mass, yielding a heterogenous echo pattern, formed in this case is thought to have been produced by adhesions between inflamed tubal structures, blood and degenerating conceptus.
Low serum beta-hcg levels can be attributed to the small number of live villi associated with the gestational sac.
Reference article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5446875/