Article by: Utkarsh Agrawal and Vedant Datta

Case Presentation:
A new case report details a 10-year-old girl patient presenting to the emergency room upon developing severe left lower quadrant pain along with nausea.
Upon examination, a sudden onset, constant pain was noted. The pain had a 10/10 severity score without any alleviating factors. At first, a case of Abnormal Menarche was suspected. But, she presented with Menarche 5 months earlier and was having normal monthly cycles since.
She gave a significant surgical history of appendectomy. Apart from that, she did not report any fever, diarrhoea, constipation, vaginal bleeding, dysuria, or trauma; and the rest of her history and labs were unremarkable.
The patient was hemodynamically stable but appeared to be in significant pain. A transabdominal ultra-sound showed a large, simple cyst in the midline pelvis measuring up to 5.6 cm superior to the bladder and anterior to the uterus.
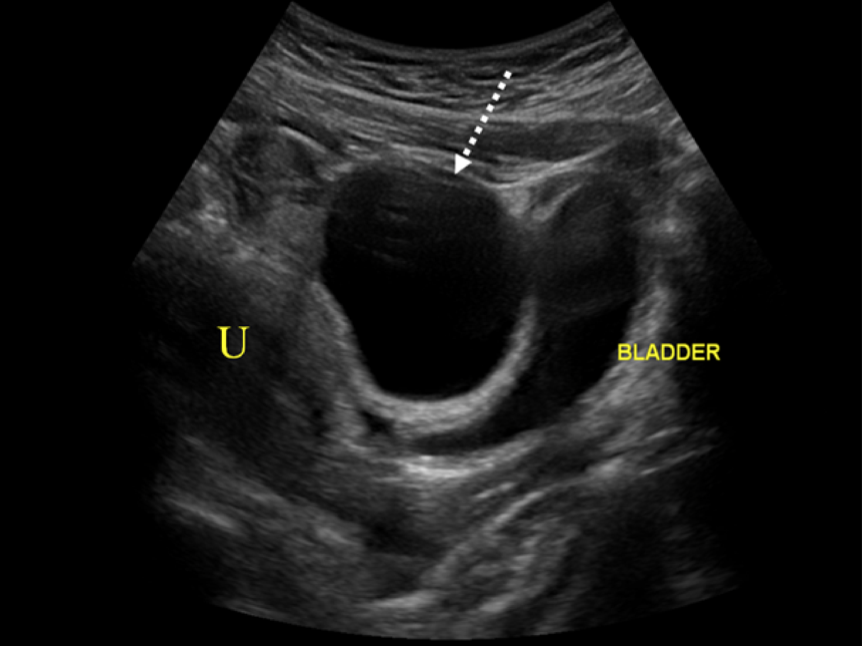
Images which demonstrate a cyst to be independent of the bladder are critical. A large cystic mass could inadvertently be identified as the urinary bladder or even a bladder diverticulum.
Careful assessment of the large simple cyst demonstrated a hyperechoic rim of tissue representing a displaced left ovary.

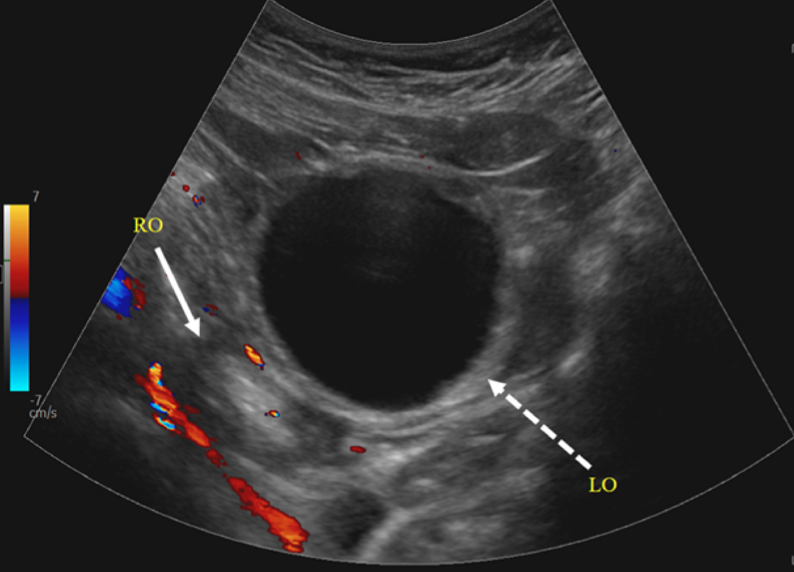
Doppler assessment of the large simple cyst and displaced left ovary demonstrated no discernible vascularity concerning ovarian torsion. The vascular flow was normal in the right ovary.
Given the patient’s findings, ovarian torsion could not be ruled out without intraoperative evaluation. Gynaecology was consulted and an emergency operative evaluation was discussed to preserve ovarian function. The patient’s mother gave consent, and the patient underwent a diagnostic laparoscopy, left ovarian detorsion, and aspiration of the left ovarian cyst.
Operative findings included a 10 cm left ovarian simple-appearing cyst with a bluish hue. Torsion was noted at the infundibulo-pelvic ligament and Utero-ovarian ligament which were successfully detorsed.



Discussion
This case reports on a paediatric patient who recently underwent menarche and presents with ovarian torsion from an ovarian cyst on the left side. However, the majority of adnexal torsion, i.e., 64%, occurs on the right side as the left side is protected by the descending colon.
The exact time needed for the vascular interruption to cause irreversible damage to the ovary is still unknown, but studies suggest a sharp decrease in ovarian function to be around 72 hours after symptom onset.
This patient presented to the emergency room 10 hours after symptom onset. Symptoms are generally sudden-onset non-radiating abdominal pain which is intermittent and associated with nausea and vomiting.
It can take around 36 hours after detorsion to see improvement in the colour of the ovary.
Due to significant edema and concern that dissection may further compromise vascular perfusion, aspiration of the cyst is on occasion safer than cystectomy, which was the case for this patient.
If needed, a two-staged procedure is an option that would allow time for the edema to decrease and reperfusion to occur, allowing for safer dissection of the cyst wall from the ovarian cortex.
Symptoms
Premenarchal patients are more likely to present with diffuse pain instead of localized pain, fever, restlessness, palpable pelvic mass, bluish/black ovary at surgery, and longer duration of symptoms when compared to postmenarchalpatients.
Premenarchal patients are thought to have elongated Utero-ovarian ligaments which may increase the risk of adnexal twisting and torsion by allowing excessive movement. The ligaments shorten with pubertal maturation.
Diagnostics
Diagnostic procedures may include pelvic ultrasound, colour Doppler ultrasound, computed tomography, magnetic resonance imaging, endorectal ultrasound, and diagnostic laparoscopy.
Pelvic ultrasound is the modality of choice when torsion is suspected particularly in premenopausal women due to the lack of ionizing radiation, and the overall diagnostic accuracy is reported to be 79% compared to 42% on CT.
Surgical management
Surgical approaches include adnexectomy, cystectomy, salpingectomy, oophorectomy, or detorsion with the aspiration of cyst fluid or cystectomy.
Oophorectomy should be avoided unless the ovary is nonviable, malignancy is suspected, or the patient is postmenopausal. Oophorectomies are also not indicated to prevent venous thromboembolism after detorsion as there is no evidence in the literature to support this practice. Use of oral contraceptive pills or depot medroxyprogesterone acetate can be considered for ovulation suppression to prevent recurrent physiologic cysts.
If a cystectomy is not performed or indicated, consideration should be made for incision and drainage of large cysts with repeat ultrasonography at 6-12 weeks.
Footnote
Ovarian torsion is an emergency that requires timely intervention with operative evaluation to preserve ovarian function and future fertility. It accounts for accounts for approximately 20 to 30% of ovarian surgeries in paediatric patients of 9 to 14 years old. Adnexal torsion is the fifth most common gynaecologic emergency. Conservative management should be strongly considered when there is no underlying ovarian pathology. This present case report shows that a swift diagnosis of ovarian torsion and timely surgical intervention can salvage and preserve ovarian function.
Credits: Volume 2022 |Article ID 9419963 | https://doi.org/10.1155/2022/9419963 Katie P. Nguyen , William L. Valentino , Duy Bui, and Honey Milestone Copyright © 2022 Katie P. Nguyen et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.