With this monthly marvel, Cutting edge brings to you some rare surgical anatomical abnormalities.
Article by: Vedant, Rahul, Vaishnavi and Manan
Design by: Manan Chawda
Rare congenital anomaly of duodenal shape
The patient presented with abdominal pain, anorexia, malaise, and jaundice a few weeks before hospitalization. Biochemical tests predicted an acute biliary obstruction. An Esophagogastroduodenoscopy was performed which detected a Vater’s ampulla tumor, and biopsy confirmed malignant histology.
The anomaly of the duodenum went unrecognized by radiologists and surgeons before surgery.
A duodenopancreatectomy with standard lymphadenectomy was performed, during which an abnormal shape of the duodenum was found:
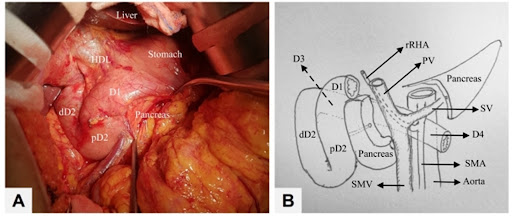
There was a change in the position of the distal half of the second part (D2), and the third part (D3).
D1 and the proximal half of D2 descended the head of the pancreas which is normal.
However, the distal half of D2 bent to the right. And it ascended upwards to the upper-right margin of the head of the pancreas. D3 went slanting downward to the left, posterior to the pancreas and portal vein.
The fourth part (D4) moved through the space between superior mesenteric artery (SMA) and abdominal aorta artery.
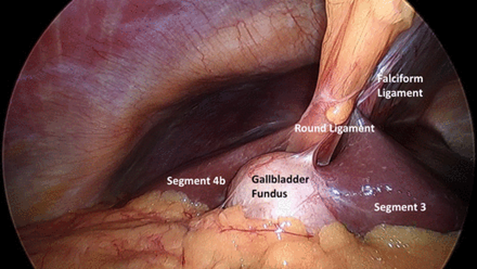
Left-sided gallbladders
Left-sided gallbladders (LSG) are a group of congenital anomalies that were described by Hochstetter in 1856. LSG consists of three types: LSG intrinsic to situs viscerum inversus (S-LSG), LSG with an abnormally right-located falciform ligament (R-LSG), or true LSG (T-LSG).
A T-LSG is located left from a normally positioned ligamentum teres hepatis (LTH) underneath the left hepatic lobe with the cystic artery crossing the common bile duct (CBD) from right to left.
Embryological explanation suggested for the existence of LSG without situs inverses describes the development of two gallbladders adjacent to the LTH during the early embryological stages. The main gallbladder on the right side of the LTH will show atrophy and eventually disappear.
Since the visceral pain fibres do not transpose with the gallbladder, a patient with T-LSG will still experience right upper quadrant abdominal pain radiating to the back with a positive Murphy’s sign with cholecystitis.
It can be diagnosed with MRI or CT-cholangiography. Several anatomical variations are associated with a T-LSG, i.e., complete, or partial situs inverses, atrophy of hepatic segment IV, duplicated or hypoplasia of the CBD, intraportal bile ducts, and abnormal pancreato-biliary junction
If T-LSG is diagnosed pre-operatively, the traditional LC port placing can be adjusted to ensure better exposure of Calot’s triangle and other critical structures.
Human Tail
On physical examination, A 9-month-old male infant was found to have a 5 cm long appendage attached to the back tip of coccyx appearing like a human tail. It was found that the size had been increasing with age and it was soft and non – tender, covered with normal skin. His muscle strength, tone and sensation were intact with normal reflexes present. The patient had no history of any abnormalities.
Plain radiographs revealed cleft vertebrae of the ninth thoracic vertebrae, and bifid rib of the fourth rib (Figure (a)). Computed tomography (CT) scans showed split cord malformations, block vertebrae of the third and fourth vertebrae, and hemivertebra of the second sacral vertebrae (Figures (b) and (c)). Magnetic resonance imaging (MRI) showed split cord malformations (Figure (d) and (e)).


With the impression of human tail coexisting with type I split cord malformations, operation of resection of the tail, removing of the septum and spinal cord untethered, was done with continuous intraoperative monitoring of sensory evoked potentials and electromyogram recording of lower extremity and sphincter muscles. The tail was elliptically excised, and the subcutaneous portion sharply dissected from the dorsal lumbosacral fascia. Despite careful inspection for a fascial defect and subfascial extension of the tail structure, none was observed, and the tail was removed enbloc
The infant was recovered uneventfully in the postoperative period. In the follow-up till 18 months, he was all right without any neurological deficit.
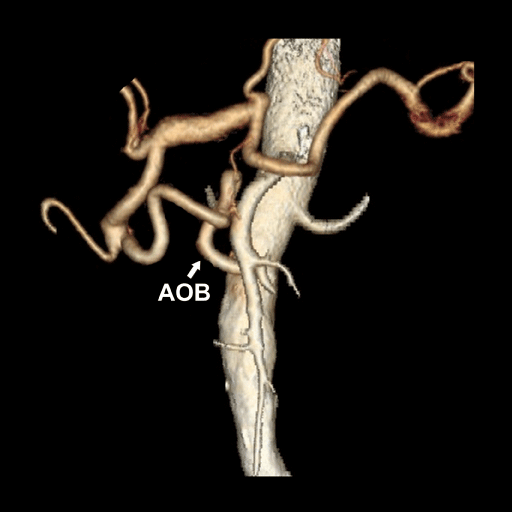
Arc of Buhler
The arc of Bühler, an anastomotic vessel between celiac artery and superior mesenteric artery, is a rare anatomic variation. Various radiologic and surgical procedures can be affected by its existence.
Only 53 cases have been described until today in the literature. The arc of Bühler enhances collateral circulation between celiac artery and superior mesenteric artery alongside with pancreaticoduodenal arcades and dorsal pancreatic artery. Computerized tomography and angiography are the main studies used for its detection and evaluation. Aneurysms of Bühler’s arc have been rarely described and seem to share common pathophysiological mechanisms with aneurysms of the pancreaticoduodenal arcades.